UCLA-led evaluation shows improved outcomes for Medi-Cal patients under a demonstration program for public hospitals
An evaluation by Dr. Nadereh Pourat found a decreased use of emergency department visits and slower growth in Medi-Cal payments for public hospitals.
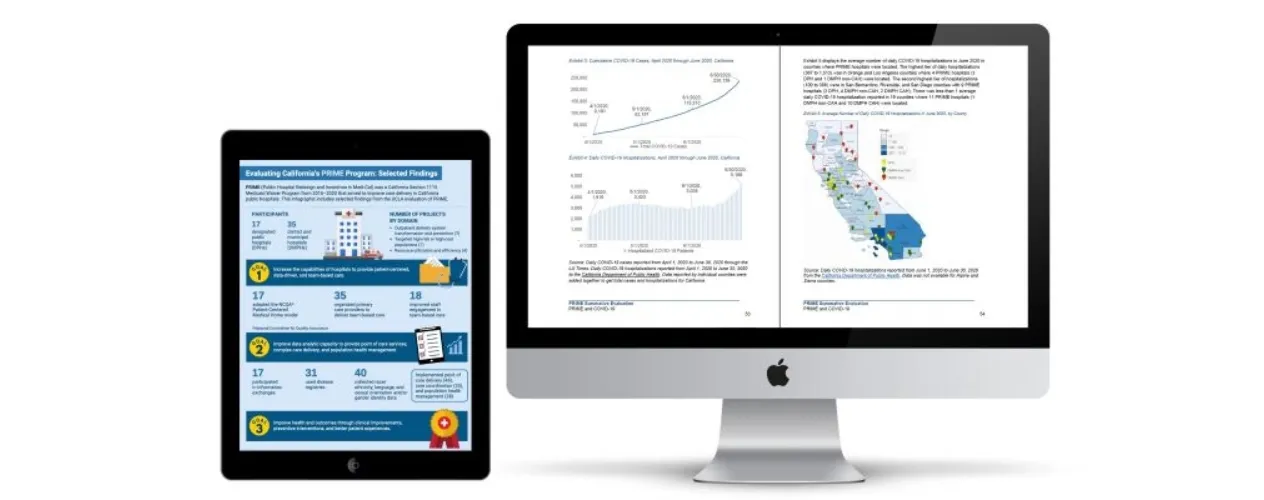
Researchers led by Dr. Nadereh Pourat, UCLA Fielding School of Public Health professor of health policy and management, have released findings from the Final Summative Evaluation of California’s Public Hospital Redesign and Incentives in Medi-Cal (PRIME) Program.
The report, issued by the UCLA Fielding School of Public Health's UCLA Center for Health Policy Research (CHPR), provides a final assessment of the five-year program’s impact on health outcomes, utilization of services, and Medi-Cal payments.
"The findings of this evaluation highlight the importance of federal funding for initiating and promoting progress in quality improvement projects," said Pourat, who also serves as director of the Health Economics and Evaluation Research (HEER) Program at UCLA CHPR, "They can be used to inform federal and state Medicaid policies to promote better care, better health, and lower costs."
Pourat's co-authors include Dr. Jack Needleman, the UCLA Fielding School of Public Health’s Fred W. and Pamela K. Wasserman professor and chair of the Department of Health Policy and Management, and Dr. Gerald Kominski, UCLA Fielding School of Public Health professor emeritus of health policy and management, along with CHPR researchers Ana E. Martinez, Anna Warrick, and Dr. Xiao Chen.
Prior reports, such as the Interim Evaluation of PRIME report, described detailed information on the program’s implementation and hospital-reported performance metrics.
PRIME was implemented by 54 public hospitals in California, including 17 designated public hospitals (DPHs) and 35 district and municipal hospitals (DMPHs), to improve care delivery, cultural competence, patient health outcomes, and to move public hospitals towards value-based care.
The UCLA CHPR research team conducted the PRIME evaluation, along with the California Medicaid Section 1115 Waiver Whole Person Care (WPC) Program and other innovative Medi-Cal programs such as the Health Homes Program (HHP).
The report findings show that PRIME hospitals had:
• Reduced hospitalizations (2.33 fewer per 1,000 patients per year among DPHs) and emergency department visits (6.32 fewer among DPHs; 15.36 among DMPHs) for PRIME patients compared with patients of other providers.
• Reduced Medi-Cal payments per person per year ($836 among DMPH; $865 among DPHs).
• Used innovative approaches and modifications to implement PRIME projects, mitigating COVID-19 pandemic disruptions.
• Improved public hospitals’ ability to participate in managed care value-based payments.
by Tiffany Lopes
The UCLA Fielding School of Public Health, founded in 1961, is dedicated to enhancing the public's health by conducting innovative research, training future leaders and health professionals from diverse backgrounds, translating research into policy and practice, and serving our local communities and the communities of the nation and the world. The school has 761 students from 26 nations engaged in carrying out the vision of building healthy futures in greater Los Angeles, California, the nation and the world.
Faculty Referenced by this Article













Dr. Michelle S. Keller is a health services researcher whose research focuses on the use and prescribing of high-risk medications.








Nationally recognized health services researcher and sociomedical scientist with 25+ years' experience in effectiveness and implementation research.






























Professor of Community Health Sciences & Health Policy and Management, and Associate Dean for Research

















EMPH Academic Program Director with expertise in healthcare marketing, finance, and reproductive health policy, teaching in the EMPH, MPH, MHA program





Dr. Ron Andersen is the Wasserman Professor Emeritus in the UCLA Departments of Health Policy and Management.






